March 25, 2026
Introducing Co-Medic Research: Identify patient populations in primary care
Max van de Ven, Stijn Bruggeman, Ruben Styl

From patient data to population research
Primary care holds a large amount of patient data, lab results, diagnoses, prescriptions, vital signs, specialist letters. Access to this data at population level has always been a bottleneck. Identifying a cohort like "patients with elevated NT-proBNP and signs of heart failure who are not receiving RAAS-inhibiting therapy" typically requires combining custom database queries with extensive manual chart review.
Co-Medic Research makes population and cohort analysis directly actionable, providing straightforward insight into the full practice population based on coded EHR data supplemented with concepts from unstructured clinical text. The result is a structured, queryable population table ready for analysis.
How it works
Define your population query
Describe the patient population you are looking for, which diagnoses, lab values, medications, or risk factors matter. Set inclusion criteria, value thresholds, and time windows to shape your cohort.
Co-Medic enriches
Co-Medic runs targeted enrichments across the patient population. Structured EHR data is matched first. Where gaps exist, the NLP pipeline processes unstructured letters and reports to fill in missing concepts.
Analyse your cohort
Review the resulting cohort in a structured population table. Each row is a patient, each column an extracted and traceable data point. Drill into individual records, refine your query, or export the cohort for further analysis.
Every data point in the practice, queryable
Each column in a population table maps to a specific type of clinical data. The system currently supports more than 20 column types, including:
LOINC-coded values, ranges, trends over time
Active prescriptions, ATC codes, dosage changes
Diagnoses coded in ICPC-2, 3BT and SNOMED-CT
Blood pressure, BMI, heart rate, oxygen saturation
Surgical history, imaging, interventions
Vaccination status and schedules
Age, sex, practice status
Active care pathways, trajectories, insurance status
Combine columns with clinical logic to flag complex criteria
Allergies, social history, family history, imaging and findings from history-taking and physical examination, ...
Enrichments: when structured data is not enough
Not every clinical finding is correctly coded. A diagnosis mentioned only in a discharge letter, a lab value buried in a specialist letter, a medication change described in free text... this is the reality of primary care data.
Data coverage across a practice population
When there are gaps in structured data, Co-Medic can run targeted enrichments to fill them from unstructured sources such as specialist letters and clinical notes.
Every enriched value links back to the source document. Nothing is a black box, you can always verify where a data point came from.
A practical example: diabetes screening
A practice wants to get a complete picture of its diabetes population. They build a population query with five criteria, Type 2 diabetes diagnosis, HbA1c, eGFR, LDL cholesterol, and metformin use, and evaluate every patient in the practice at scale.
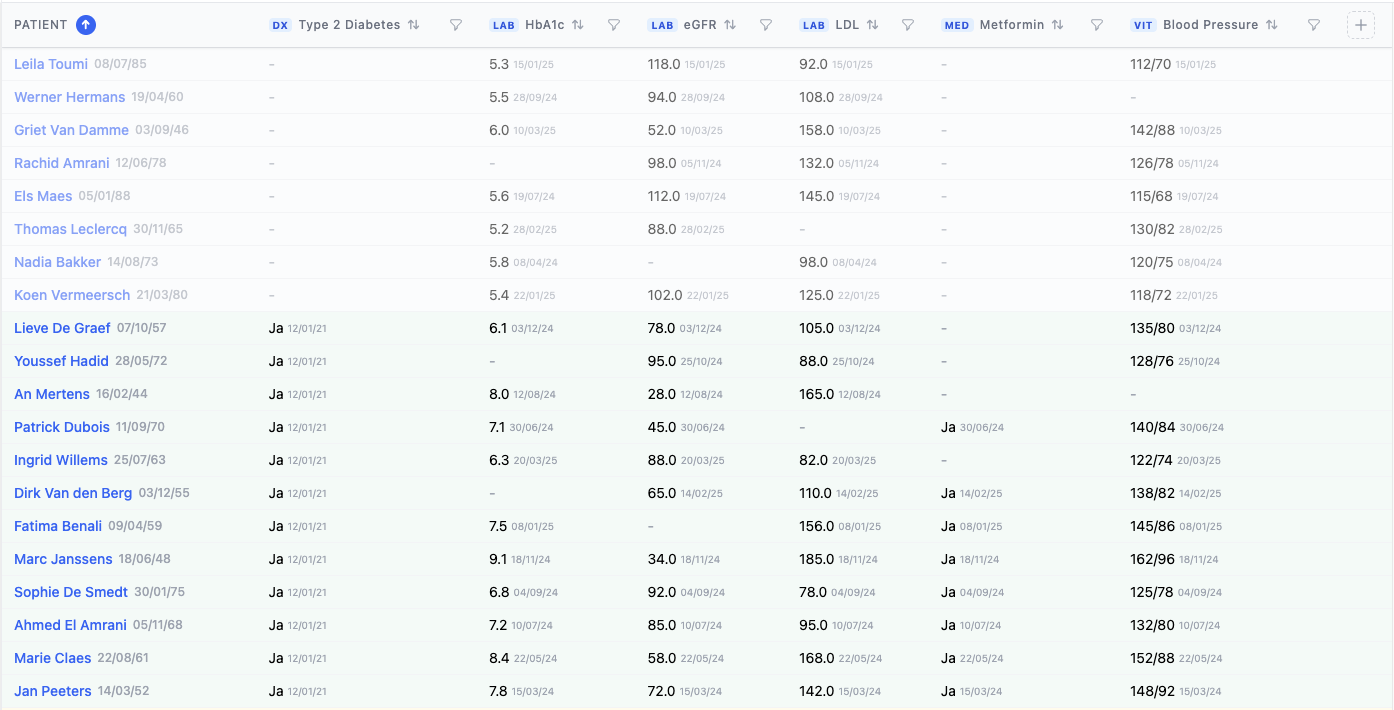
Each column retrieves data from the patient's clinical record, lab results via LOINC code, medication via ATC classification, and diagnoses via ICPC-2 and SNOMED-CT. Where data is missing, Co-Medic can run targeted enrichments to extract values from unprocessed letters and reports.
From question to cohort
You do not need to configure every criterion by hand. Co-Medic Research includes an agent that helps you build population queries through natural language. Describe your research question: "Find patients with CKD stage 3+ who are not on SGLT2 inhibitors without a recorded contraindication", and the agent translates that into criteria, enrichments, and thresholds.
Private beta
Co-Medic Research is currently available for selected partners and research projects. If your practice or research group wants early access, please feel free to get in touch.
Get in touchWant to explore Co-Medic further?
Connect with our team or keep reading more insights from our blog archive.
Related articles

Feb 27, 2026
From letter to structured care data
How incoming specialist letters are automatically converted into coded, searchable clinical data for the general practitioner.
Read more
Feb 5, 2026
Chronic kidney disease: from underdiagnosis to overview with population management
CKD is often insufficiently followed up in primary care. Population management helps identify and follow patients according to guidelines.
Read more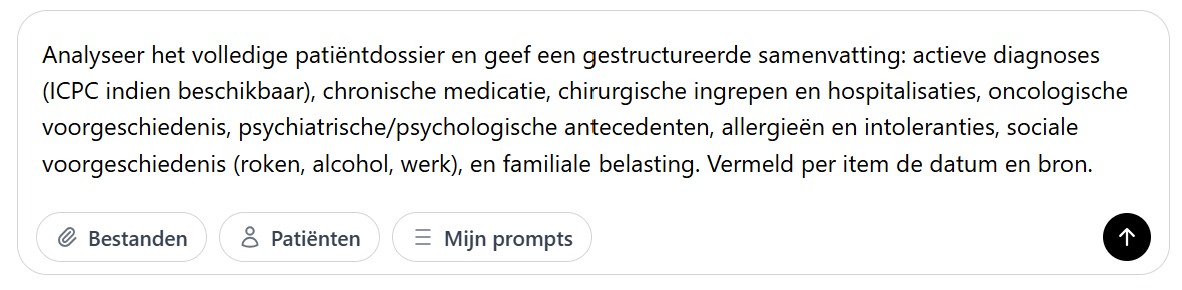
Jan 27, 2026
How Co-Chat relieves daily administrative tasks
Dr. Bram Spinnewijn shows how he writes referral letters during consultations with Co-Chat, without GDPR concerns.
Read more