Population management for primary care
See who's missing follow-up, before it becomes a problem.
Co-VIHP brings your practice data together into one population overview. Identify at-risk groups, follow up on care pathways and plan chronic care proactively. No extra coding, no manual searching.
Population overview from your own practice data
Rewatch our webinar on population management in primary care
Watch the recordingOne overview
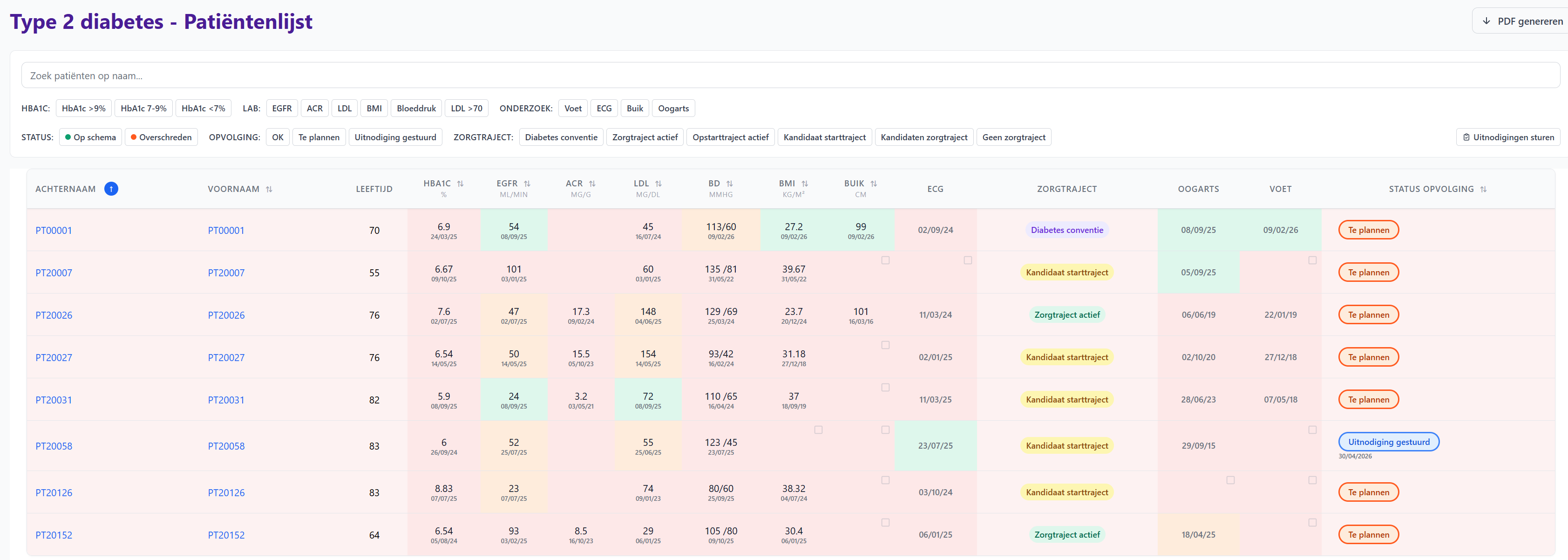
From patient list to action list
Co-VIHP shows, per care pathway, who is on track and who is due for follow-up. Every parameter comes from your own records and links back to the source document.
Care pathway candidate
Chronic kidney disease
| Patient | Most recent eGFR | Previous eGFR | Proteinuria | Follow-up status |
|---|---|---|---|---|
| Maria Peeters | 29.0 | 29.0 | 60.0 | OK |
| Jef Claes | 37.0 | 39.0 | - | OK |
| An Mertens | 34.0 | 32.0 | - | OK |
| Karel Willems | 24.0 | 27.0 | - | To plan |
| Rita Jacobs | 30.0 | 32.0 | - | To plan |
Example view with representative data.
The impact
Proactive care, organized at practice level
For your practice
- Population overviews replace days of manual searching through records
- Task delegation to the practice nurse or VIHP becomes feasible
- Care pathways are correctly identified and started
For your patients
- At-risk patients are found earlier, even when the diagnosis only appears in free text
- Prevention and guideline-based follow-up instead of avoidable complications
- Chronic care is planned instead of followed up reactively
Applications
One method, multiple care pathways
Diabetes & renal insufficiency
Bring lab values, diagnoses and follow-up together in one overview per care pathway.
- Care pathway monitoring
- At-risk person identification
- Evaluation of medication
Osteoporosis & heart failure
Apply diagnostic algorithms to structured data to detect conditions such as heart failure.
- Complex queries
- Structured secondary care data
Prevention & screening
Identify patients who are missing a recommended screening or follow-up, based on existing record data.
- Identification of follow-up gaps
- Guideline-based screening
Additional conditions and screenings are added step by step.
For whom
Practice nurse 'VIHP'
Preparation & follow-up
Prepare consultations, follow protocols, screen at-risk patients.
General practitioner
Supervision & validation
Chronic care follow-up, identification of gaps.
Practice manager
Organization & reporting
Task distribution and team coordination.
Our vision
"We are moving towards a future where general practitioners are no longer coders. Relevant data is automatically structured from letters and notes. This allows organizing chronic care at practice level with insights from structured data."
Co-Medic
Tailored to your practice?
Discover how Co-Medic can be adapted to the specific needs of your practice. Schedule a conversation with our team.